On Thursday, 4th July, the nation will head to the polling stations to decide the next government. After a turbulent 14 years under Conservative rule, marked by complexities ranging from Brexit to COVID-19, the nation now has the chance to choose whether to continue with the status quo or opt for a different direction.
At our foundation, we have reviewed the policy wishlists set out by the three main parties: Conservatives, Labour, and Liberal Democrats. However, despite their broad statements about addressing structural inequalities in healthcare, we are disappointed by their lack of focus on how these policies will impact Black, Asian, and minoritised ethnic communities, which make up 18% of the population in England and Wales.
Physical Health Inequalities
Our 2023 research with UCL and Doctors of the World highlighted the disproportionate impact of the COVID-19 pandemic on ethnic minority and migrant communities. We found that Black men were twice as likely to die from COVID-19 compared to White British men during the first wave of the pandemic, with the likelihood increasing by 70% during the second wave. Additionally, people of South Asian heritage, who constitute 1 in 13 of the population, accounted for 1 in 10 fatalities. These statistics underscore systemic inequities that contribute to differential health outcomes. The lack of attention to these issues in the party manifestos suggests that the political establishment is not being held accountable for how COVID-19 has exacerbated racism and the ongoing role of racism in people’s lives.
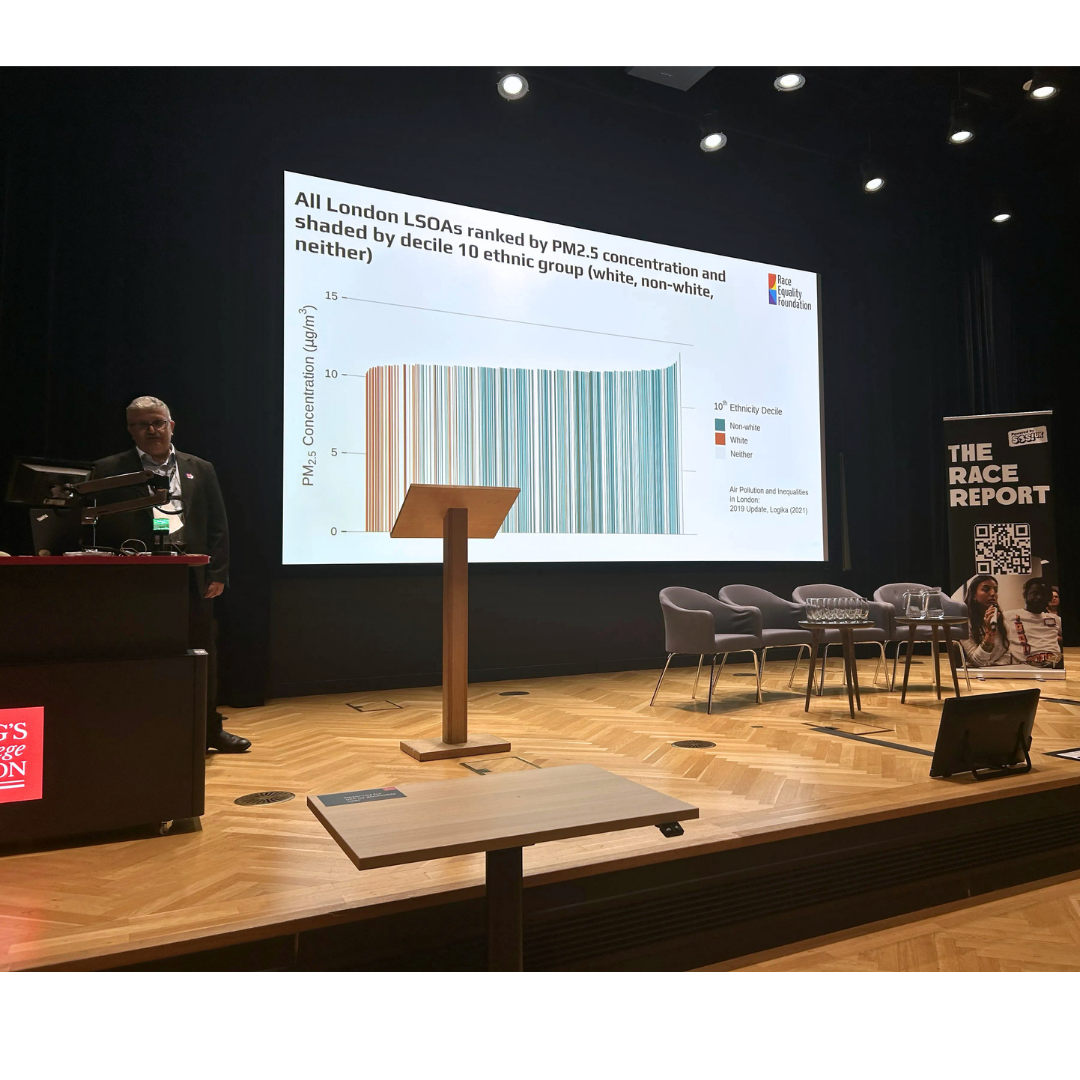
Just last week, we launched the Make Health Equal campaign with Health Equals, which highlights the role of access to healthy food, affordable quality housing, improved air quality, and access to green spaces in reducing health inequalities. Comparatively poorer access and experiences affect Black, Asian and minoritised ethnic communities disproportionately, contributing to poorer health and well-being.
Further research conducted by our foundation in 2023 found that specific groups within the Black, Asian and minoritised ethnic population have significantly lower life expectancies. For instance, the average age of death for people with a learning disability from an ethnic minority is 34 years, just over half the life expectancy of their white counterparts, who live to an average of 62 years.
Mental Health Inequalities
Beyond physical health, our research reveals that Black, Asian and minoritised ethnic communities are at higher risk of mental ill health and are disproportionately impacted by social determinants associated with mental illness. For example, people from African Caribbean communities are three times more likely to be diagnosed and admitted to hospital for schizophrenia than any other group. Irish Travellers are six times more likely to die by suicide than non-Travellers.
Evidence shows that Black, Asian and minoritised ethnic communities are less likely to access mental health support in primary care (e.g., through their GP) and more likely to end up in crisis care.
Addressing the Root Cause: Racism
Historical and current racism is the root cause of ethnic inequalities in both individual and area-level socio-economic status and health. Ignoring racism as the main factor leading to these inequalities will only partially address the problem. Importantly, it also means ignoring what can be changed. A national race equality strategy with a clear plan to tackle ethnic inequities in health and socio-economic conditions must be produced and implemented to prevent the ongoing production and reproduction of these inequities.
However, it’s clear that reducing health inequalities isn’t seen as a vote-winner. Parties are focusing on sensationalist, headline-grabbing policies such as illegal immigration. If we get it right for Black, Asian and minoritised ethnic communities, we will positively impact other communities as well.
We will continue to advocate for addressing health inequalities, as not tackling them is not cost-free.